Pioneering FUE Hair Transplant Adaptation for Asian Hair: A 16-Year Journey of Innovation
Home » Our Innovation – FUE In Chinese Population
Our early application of the European FUE techniques revealed significant limitations. The protocols were designed for Caucasian hair follicles, which differ markedly from the thicker, often curlier follicular structure and denser scalp tissue of our East Asian patients. This anatomical mismatch led directly to suboptimal clinical outcomes: unacceptably low graft survival rates, poor yield, and dissatisfied patients.
This challenge catalyzed our commitment to innovate. We systematically analyzed these failures, adapted the instrumentation and technique, and documented our findings. As validation of our work and to guide other surgeons, we became the first clinic to publish our adapted methodology for the Chinese population in the ISHRS’s peer-reviewed medical journal, Hair Transplant Forum International, with our paper “Follicular Unit Extraction: Experience in the Chinese Population.” This publication not only supported our clinical claims but also established a foundational reference for performing FUE in Asian patients.

Our clinic pioneered Follicular Unit Extraction (FUE) for East Asian patients, recognizing that European protocols failed on thicker, curlier Asian hair. After pausing services in 2007 to research and adapt, we developed a modified technique. This foundational work evolved into our proprietary FUE-HD method, designed specifically for the anatomical and aesthetic needs of the Chinese population.
Not without significant modification. The global FUE technique, developed primarily on Caucasian hair, often yields poor results on Asian patients due to fundamental differences in hair shaft thickness, follicular curvature, and scalp density. A specialized approach is required to ensure high graft survival and natural aesthetics for East Asian patients.
Asian hair presents distinct anatomical characteristics that complicate standard extraction:
Thicker Hair Shafts: Require careful punch size selection to avoid collateral damage.
Subcutaneous Curvature: Follicles often have a hidden “J-hook” or “S-shape” beneath the skin, increasing transection risk if not approached correctly.
Denser Scalp Tissue: Offers more resistance, demanding specialized motor settings and extraction angles.
Aesthetic Standards: Hairline design and density goals often differ, requiring a tailored aesthetic approach.
Guided by the principle “First, do no harm,” we undertook a methodical research and development process.
Recognition of Failure (2006-2007): Initial attempts using European techniques resulted in low graft survival and poor patient satisfaction, prompting us to pause all FUE services.
Dedicated Research (2007-2008): We engaged in advanced global training and focused on understanding Asian follicular anatomy to identify the root causes of graft transection and poor yield.
Technique Development & Publication (2008 onward): We successfully adapted the protocol and published our modified techniques in international journals and textbooks (e.g., Hair Transplant Forum International, 2009) to share knowledge and prevent other surgeons from repeating our early difficulties.
The culmination of this work is a refined, high-precision surgical protocol.
FUE-HD (High-Density FUE): Our proprietary technique uses custom-sized punches and precise motor settings to navigate the unique curvature and density of Asian follicles, maximizing intact extraction.
Optimized for Natural Density: The method allows for safe, dense packing that meets the common aesthetic preference for fuller coverage among Asian patients.
Proven Track Record: Built on thousands of cases over 16+ years, providing reliable, natural-looking outcomes for the local population.
The learning curve is significant. A surgeon unfamiliar with the nuances of Asian follicular anatomy is more likely to encounter:
Higher Transection Rates: Damaging the precious, finite donor grafts.
Suboptimal Yield: Harvesting fewer usable grafts than planned.
Unsatisfactory Aesthetics: Creating a hairline or density that appears unnatural for the patient’s ethnicity.
Asian Hair is Anatomically Distinct: Successful FUE requires specific adaptations for thicker, curlier follicles and denser scalp tissue not typically addressed in standard protocols.
A History of Pioneering Adaptation: Our clinic pioneered and published modified FUE techniques for Asian patients after initial failures with European methods, establishing a foundation for regional practice.
Specialized Technique Matters: Our FUE-HD protocol is engineered from the ground up for Asian patient characteristics, prioritizing graft survival and natural density.
Experience is Non-Negotiable: Given the technical complexity, choosing a surgical team with extensive, documented experience in Asian FUE is critical to protecting your donor supply and achieving a satisfactory result.
Published in : ISHRS FORUM International. Vol 19:1, Jan/Feb 2009
In1988 Masumi Inaba in Japan introduced the use of 1mm punch in extracting individual follicular unit. In 2002 Rassman refined the procedure and named it Follicular Unit Extraction (FUE) or FOX procedure (FOllicular unit eXtraction). FUE serves as an alternative other than strip in donor harvesting (1). It attracts attention of those who desire hair transplantation but are turned off by a linear donor scar.
Being a blind technique, the number of grafts is limited by a high transection rate. Over the years many different FUE techniques have evolved to overcome this problem (2)(3)(4). A 5-steps personal approach will be described in part one of this chapter.
The real problem of FUE however is the depletion of donor grafts for future sessions. Part two will outline the considerations when offering FUE mega-session to those Asian subgroups who have a low hair density and low hair-to-graft ratio (e.g. Chinese, Japanese, Thai) (5,6).


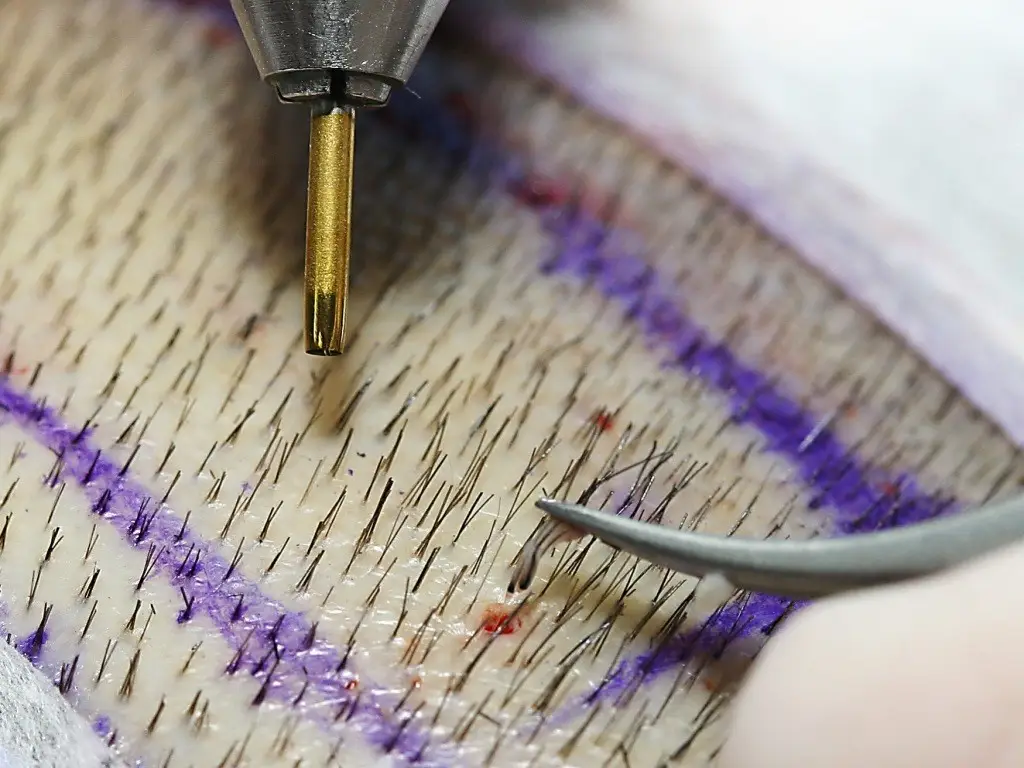


FUE Round Punch 0.75 to 0.8mm should be reserved for 1-hair FU. Size 1.0mm can be used for most 2- and 3-hair grafts. Larger 1.2mm punch, with a potential to leave scar and transect adjacent follicles, should be avoided (1).
Vari-handle is recommended as punch holder for 3 reasons
Curved forceps provides a larger contact area for a better grip of graft. A second pair of straight forceps is needed for difficult extraction.
Surgical loupes provides good visualization.
Magnification higher than 2X may cause more
eye-strain.
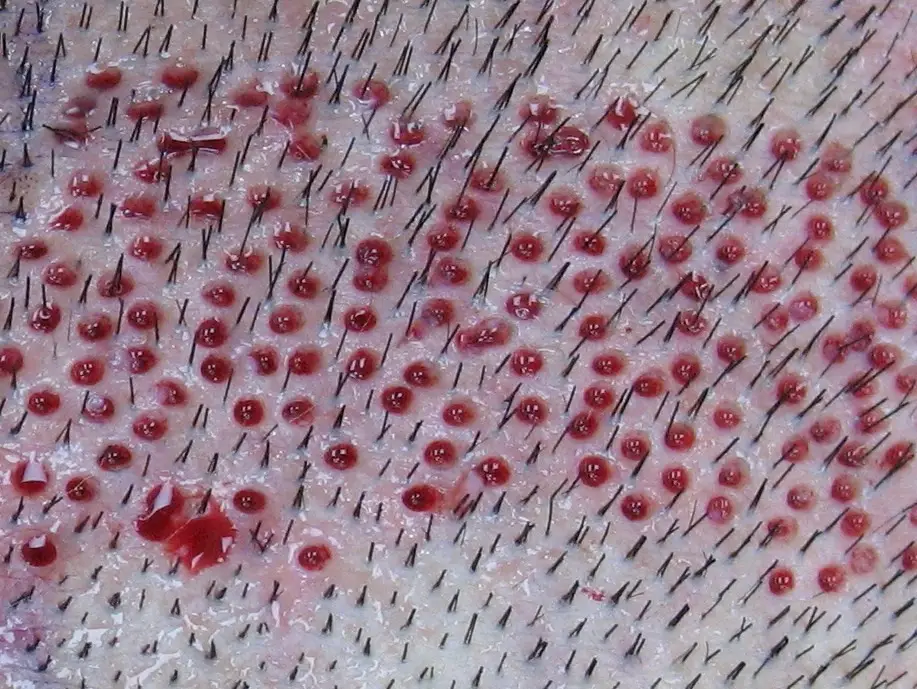
Moist dressing material instead of gloved finger should be used to collect extracted grafts (Fig 4) before transferring to a Petri-dish with cool saline (7).
Grey or white hair should be colored before surgery. FOX test has been advocated for patient selection especially in megasession (8). In real practice it is rather time-consuming and unreliable. What initially appears to be difficult may turn out to be easy extraction after the surgeon adapts the technique to cater for the angle and direction of the follicles. The entire donor site should be trimmed leaving behind 0.3-0.5cm of hair above the skin to guide the punch. Those reluctant to shave must have kept hair long enough to cover one or two trimmed windows.
Scalp laxity should be assessed (9). Very tight scalp alerts the possibility of underlying idiopathic tissue fibrosis which necessitates deeper scoring.
Patient’s comfort must be ensured as FUE takes many hours. The patient should lie in a prone position with the surgeon sitting either by the side or at the end of the table.
Inspect the hair at the occiput and parietal areas. The surgeon should start at an easy area to gain confidence.
The patient’s neck should be flexed when harvesting the inferior donor area. Here the hair usually exits at flat angle and stretching the scalp helps to erect the follicles.
The ‘safe margins’ of the donor area should be marked to avoid picking up non-permanent hair. There is no fixed rule in defining the safe donor areas. However Unger and Alt’s recommendations may be used as guideline (10).
Looking for grafts at the end of procedure is frustrating. One practical tip is to divide the marked donor area into small blocks of similar sizes.
N = The planned number of grafts
n = The number of blocks
N / n = The number of grafts to be harvested per block.
If this number cannot be obtained in a defined block, the surgeon should prepare to expand the donor area or accept lesser grafts.
L.A. of personal choice should be injected below and along the inferior border. Tumescence should not be injected as routine. The ease of extraction must first be tested with and without tumescence. It should be injected intra-dermally a small area at a time, and away from ‘holes’ to avoid spilling.
Graft selection
Straighforward FUE requires only 2 steps – scoring and extraction (11). When extraction is difficult with high transection, a 5-steps approach is necessary.
Three different tools can be used to free the follicle from any deep tethering before re-extraction.
These two steps are repeated until the graft is removed.
For these population the difficulties in FUE usually arises from a discrepancy between high demand (14)(15)(16)(17) and low supply of donor hair (5)(6). There are two ways to increase the number of grafts but at a higher risk for complications:

Images & Information shown are for reference only
Information on this website is provided for general educational purposes only and does not constitute personalized medical advice. It is not intended to promote our service or imply superiority over another.
Individual results in hair restoration vary significantly and no outcome can be guaranteed. The before-and-after images shown represent possible results — not promises. We recommend seeking independent medical advice to discuss your options … Read More
Paragraph

Pre-Consultation Review
If you want to get a personalized answer from our medical team, you can reach us using this form here. We will cantact you as soon as possible.
Our practice adheres to guidelines established by leading international organizations in Hair Restoration.
International Society of Hair Restoration Surgery is the leading global medical association that establishes international practice standards and patient safety protocols.

The American Board of Hair restoration Surgery represents the highest standard. To maintain rigorous certification requirements the physician must demonstrate surgical expertise.
Worls FUE InstituteI serves as the premier educational body focused exclusively on Follicular Unit Extraction methodology. The institute ensures consistent application of safe FUE.