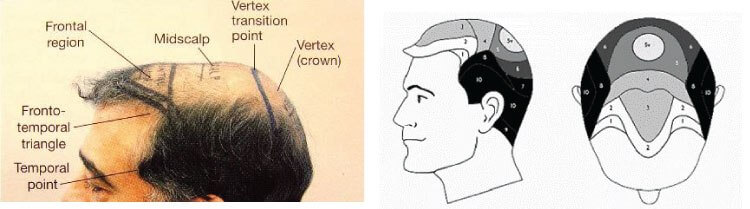
Hair loss on the crown ( also known as the vertex ) is one of the most common patterns of male androgenetic alopecia. It’s primarily driven by genetics and the hormone dihydrotestosterone ( DHT ), which gradually miniaturizes hair follicles in this region.
But crown balding isn’t just a cosmetic issue — studies have shown a possible link between vertex baldness and cardiovascular disease. Research suggests that men with significant hair loss at the crown may have a higher risk of coronary heart disease, especially if the balding starts early.
One notable physical sign that may correlate with this risk is a crease in the earlobe ( called Frank’s sign ). While not definitive, the presence of this diagonal crease has been associated with atherosclerosis in several studies, and when seen in men with crown baldness, it may point to underlying vascular issues.