Transplanting a graft from one site to another does not guarantee good result. As damaged graft cannot re-grow, the surgeon must pay attention to every step and every details of the procedure. On average 85-92% of grafts survive after transplant and grow new hair.
2 possible ways a graft can be damaged or even killed – the X-Killing Factor and the H-Killing Factor.
“X” stands for unknown. The term was first described by Dr Shield (Australia) in 1984, when the reduced hair growth was unexpected and unexplained. In early years this X-Factor only accounts for a very small 0.5-1% of all no growth. With the advance and standardization of surgicial techniques, X-Factors now accounts for the majority of unsatisfactory results.
It is of our opionion that such “unknown” factors are in fact biological damage to the grafts which takes plce during and after the procedure, including:
“H” stands for human. Poor growth is caused by a breach of protocol. H-factor may occur before, during, and after the procedure. The result of a hair transplant procedure cannot therefore be guaranteed.
Predisposing Factors That Compromise Result include:
Grafts are injured During Procedure:
Transplanted Follicles are injured after the procedure
A hair follicle is a living tissue. A lot of things take place after the follicle is planted into the new site. Understanding of the natural histochemical process is crucial, as a better graft survival means a better outcome.
After the graft is harvested from the donor area, it is placed in a storage solution for preservation until implanted in the recipient area. Its original blood supply is detached. Oxygen is depleted and waste products begin to accumulate. The ability of the graft to receive nutrients from the recipient site and undergo revascularization (formation of new blood vessels) therefore determines survival.
After the graft is inserted into one of the slits, the wound healing process immediately takes place. There is a cascade of cellular activities – edema ( swelling ), erythema ( redness ), hair shedding, new hair formation, and the revascularization of the hair graft.
At Dr. Bertram Hair Transplant Centre, our approach is built around one core principle: quality matters more than quantity. Every step of our procedure is carefully designed to maximize graft survival, ensuring that each transplanted follicle has the best chance to grow strong and last a lifetime.
After a person is born, there will not be an additional hair follicle. The permanent hair follicles at the back of our head, the donor site, are invaluable and cannot be replaced. Many people expect hair follicles to be cloned, but the date of success is an unknown. The priority is to minimize the trauma of hair follicles during the process of hair transplantation.
Over the past 50 years, many studies have been conducted to look at the actual survival rate of transplanted hair, and the percentage growth, reporting the following findings :
The final result of the hair transplant procedure depends on how many grafts actually regrow. Dr Beehner commented that the percentage of graft survival depends on the skill of the surgical team more than anything. In another word, the skill and experience of the surgical team is one of the most important factors in arriving at satisfactory result.
The doctor and the staff should not just focus on extraction, but also on how to keep it growing after transplanting into another site. Taking out a graft cannot guarantee its growth unless the H-Factors and X-Factors are looked into. We therefore saw the importance to improve graft survival.
When more grafts survive, less is required to complete the job. As most hair transplant centers charge “per graft transplanted” not “per graft survives”, a higher survival will bring the cost down. Having say that, money cannot buy back a wastage of good donor hair follicles.
Center A |
Center B |
|
|---|---|---|
| Cost per Graft (HKD) | 25 | 25 |
| No of Graft Required | 2,400 | 2,400 |
| Total Cost (HKD) | 60,000 | 60,000 |
| Transection Rate (Graft damage) | 20% | 2% |
| No. of Damage Graft | 2,400 X 20% = 480 | 2,400 X 2% = 48 |
| No. of Intact Graft | 2,400 - 480 = 1,920 | 2,400 - 48 = 2,352 |
| Actual Cost per Graft (HKD) | 60,000 ÷ 1,920 = 31 | 60,000 ÷ 2,352 = 25.5 |
CONCLUSION : A high transection rate increases the cost per graft.

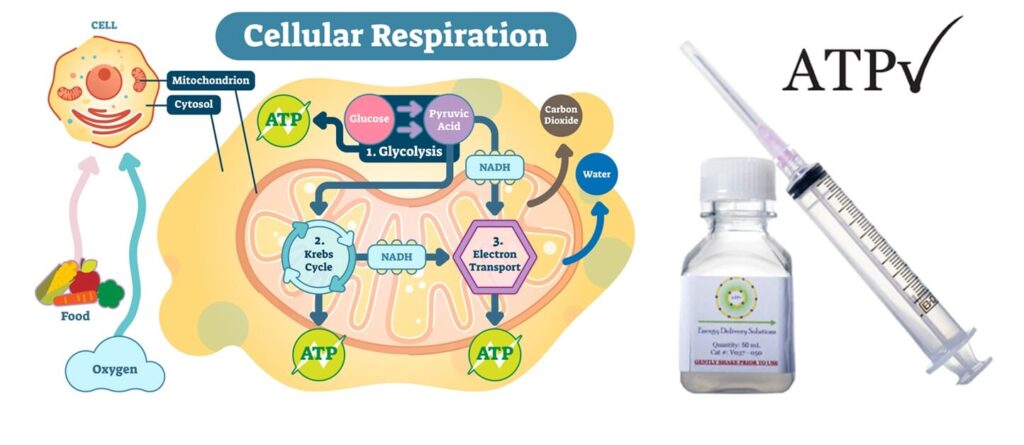
ATP (Adenosine triphosphate) is an energy molecule that catalyzes a variety of important cellular reactions in our bodies. The lack of ATP can cause cell damage and eventual cell and tissue death. Because the creation and regulation of ATP requires oxygen, tissues deprived of oxygen often experience ATP loss and become damaged. Because of this, ATP becomes crucial for patients healing from wounds; especially surgical wounds.
The usual kind of ATP solution in a vial is very cheap but the use is limited, as aqueous solution cannot be absorbed into cells.
In 2002, Dr. William Ehringer a Professor at the University of Louisville, School of Medicine, discovered a method to encapsulate and deliver ATP to cells. After 10 years of research the final formulations were identified – Lyposomal ATP. In 2012, Dr. Ehringer founded Energy Delivery Solutions in manufacturing ATP for use in post-surgical patients, patients with delayed wound healing, and in hair restoration.

Experiments by Dr Cooley and Dr Pathomvanich our Medical Advisor showed that, in hair transplant surgery, Lyposomal ATP allows for quicker healing and better hair transplant yields. In 2015 Dr Bertram Ng met with Dr Ehringer founder of Energy Delivery Solutions. Dr Ehringer and Dr Cooley. Both recommended:
1. Store grafts in ATP-containing storage solution
2. Spray ATP Formulation at home onto the recipient scalp first 48 hours, up to 5 days
Clinical trials on selected subjects for over a year revealed very impressive result. Since October 2016 we provide Lyposomal ATP to all patients routinely. As Lyposomal ATP has only a very short half life, we have to import from the state every few weeks. The benefit is well worth the extra efforts and expenses.

The Tricomin Follicle Spray from USA which contains Copper Nutritional Complex for use after hair transplant. The preparations we are using are fully imported from USA to ensure quality.
Hair transplants can initially traumatize the scalp and can result in a temporary hair loss during the first 4 months (this is known as shock loss). Some patients may experience swelling in the transplanted area. The transplanted donor follicles can also experience difficulty adapting to their new environment. Clinical studies have demonstrated the following beneficial effects of laser when use in conjunction with hair transplant.
Laser hair therapy stimulates the mitochondria in cells to increase the production of adenosine triphosphate (ATP). ATP is the form of energy used by hair cells to grow imto follicles. Abundant energy supply is critical when dealing with weakened and traumatized hair follicles.

Laser hair therapy devices have been used by thousands of hair transplant centers all over the world (such as Bosley and HairClub). However handheld contraptions made with cheap Light Emitting Diodes (LEDs) are worthless when it comes to energizing the base of hair follicles. Technologically advanced device with the FDA-cleared is now available in our center for use after hair transplant.
A 20 minutes of treatment is able to revive the mitochondria of hair cells. This can result in stronger hair follicles with a higher probability of surviving the operation. These extra amounts of “survivor” hair grafts will eventually grow into healthy, terminal hairs.
Graft transection occurs when a hair follicle is accidentally cut or damaged during the harvesting or implantation process in a hair transplant. This can happen if the angle or depth of the instrument used is incorrect, severing the follicle’s lower portion, which contains essential stem cells and the dermal papilla.
Once a follicle is transected, its ability to regrow healthy hair is significantly reduced – or lost entirely – leading to poor graft survival and wasted donor resources. Minimizing transection requires precision, experience, and the use of fine instruments under proper magnification. That’s why surgical skill and technique play a critical role in achieving lasting, natural-looking results.
Graft Survival After Partial Transection
Removing too much tissue around the hair follicle is also a form of physical injury. Stem cells responsible for follicular re-growth is located at the tissue surrounding the graft.
Seager reported in 1997 that Chubby Graft ( more fat ) survives better than Skinny Graft ( less fat ). In 2010 Beehner commented that the differences in survival is that the stem cells are retained in chubby grafts but trimmed away in the skinny grafts
Dehydration causes serious graft damage. Deleterious changes in cell integrity when follicles are left to dry for more than 5 minutes (Gandelman). When grafts are exposed to air for more than 10 minutes, more than 6% will die. After 20 minutes survival markedly decreases (Kim)
It may take 4–8 hours to complete the insertion. The elapsed time is critical for hair growth and survival because increased time results in decreased survival. As oxygen is depleted and waste products such as carbon dioxide, sugar, and urea begin to accumulate, a newly planted hair graft will be acidotic.
The first 48–96 hours after implantation is critical. If the circulation cannot be re-established (the primary inosculation) to correct the metabolic imbalances, the hair graft won’t survive and could die.
Duration After Extraction (hour) |
% of Growth |
|---|---|
| 2 | 95 |
| 4 | 90 |
| 6 | 86 |
| 8 | 86 |
| 24 | 79 |
From the table you can see that graft survival to 90% after 4 hours. So after 4 hours 10% of the extracted grafts will not grow hair. This is a wastage as the donor hair is limited in a life time.
This is a form of physical injury. Study had shown that all frozen graft will die. Domestic-grade refrigerator may have temperature fluctuation. If the fridge temperature is set too low it may drop below 0°C and kill grafts without knowing. From studies there was no significant difference in survival within 6 hours, whether the grafts were stored in room temperature or 4 °C (Kim)
• Store graft at room temperature if procedure can be complated within 4 6 hours
• Use a special storage solution ( Hypothermosol ) to store grafts in the fridge
• Try to complete implantation within 6 hours
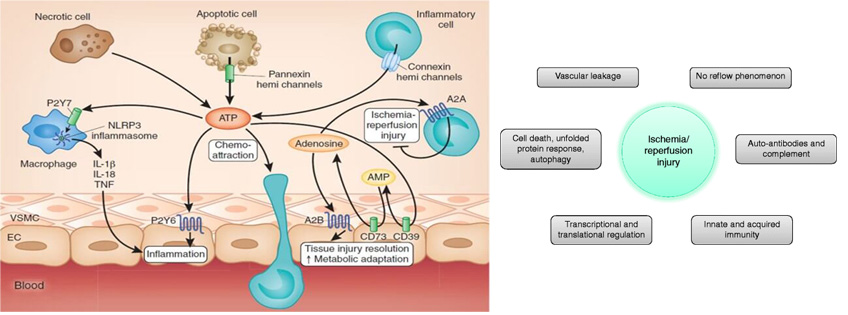
After a period of low oxygen, when the grafts are implanted and suddenly re-exposed to oxygen, they may form free radicals. These free radicals may cause cell injury and suboptimal growth, and is known as “Ischaemic Reperfusion Injury or IRI” on Re-implanted Graft.

Transplanting a graft from one site to another does not guarantee good result. As damaged graft cannot re-grow, the surgeon must pay attention to every step and every details of the procedure.


From consultation, surgery, to aftercare, you will receive continued personal care by our doctors, not just consultants.
Have a question? Please feel free to call our friendly customer service.




International Accreditations
Recognized by leading global medical bodies, our clinic stands as one of the most qualified and internationally accredited hair transplant centers in Hong Kong and mainland China. We are proud to uphold the highest standards in medical ethics, safety, and surgical expertise.
Hair transplant is the ultimate solution to restores hair, but not everyone is good candidate.
Our online assessment helps determine if these procedures suit you, saving you time and costs.








